|
How do I know if my infant needs a cranial remoulding orthosis? There are certain signs that may indicate that your infant needs a cranial remoulding orthosis. However, please keep in mind that some degree of asymmetry in the skull is normal for everyone, so it is the magnitude of the asymmetry that indicates whether treatment with a cranial remoulding orthosis is warranted. If you recognize that your infant’s face is not symmetrical, their head is higher or wider than normal, or that there is flatness on the back side of their head, you may want to visit your physician for further assessment. After 2 months of no or very slow improvement from a physiotherapist or chiropractitioner your baby should be brought in for an assessment. What is the ideal age for cranial remoulding orthosis treatment? The best age for treatment is between 4 and 7 months when the skull is growing at the fastest rate. However, cranial remoulding orthoses can be used successfully between 3 and 18 months of age. Caregivers should try to reposition the baby for at least two months prior to initiating treatment with a cranial remoulding orthosis unless the infant is older than 7 months. At this point, infants can reposition themselves, and caregiver efforts to reposition are often futile. What if my paediatrician tells me that my infant’s head shape will correct on its own? Historically, many head shape deformities present at birth disappeared within about 6 weeks because babies were placed in several different positions during the day and slept on their tummies at night. Since the Back to Sleep program was initiated in 1992, these head shape deformities often persist because babies sleep on their back all night and spend extended time on their backs during the day in infant carriers/ prams, swings, car seats, etc. Parents must be vigilant about changing the infant’s position more than in any other period of child rearing. Babies that spend most of their time on their backs in the early months roll and crawl later than usual, which results in even more time before the infant can actively reposition themselves. The best way to help your infant’s head correct “on its own” is to place your infant in a variety of positions during the time your infant is awake and supervised. This will encourage your infant to actively move their head through a full range of motion, strengthen their neck, shoulder and trunk muscles, and minimize pressure on the back of the head. More suggested repositioning activities are available in “Tummy Time Tools”, a document that can be downloaded from Orthomerica’s website. It is possible that your efforts to reposition your infant will be rewarded with a more symmetrical head shape that does not require further intervention. However, if your infant’s head does not change after two months of alternate positioning, make sure your paediatrician understands that you have tried prone and other positions to help make the infant’s head more symmetrical, and the skull has not corrected. Then ask your paediatrician if your infant would benefit from a cranial remoulding orthosis, and/or request a referral to a craniofacial specialist. Why is treatment more effective between 4 – 7 months than at other ages? Even though the head grows fastest during the first 3 months of life, this time period is best spent actively repositioning your infant to encourage more symmetry. Between 4 and 7 months of age, the head grows about 1 cm per month*, and this rapid growth can be harnessed within the orthosis to produce rapid change in the desired direction of growth. At this point, the infant is starting to develop more head control and can tolerate the additional 6-8 ounces of weight from the helmet. It is actually the infant’s own growth that is the most active part of any CRM orthotic treatment program. The orthosis is specially designed to make total contact in the areas of the skull where growth needs to be curbed and allow space in the areas where growth is desirable. Between 8-12 months, the skull still grows quickly, but the rate is reduced to 0.5 cm per month*. Between 13-18 months, the rate drops below 0.5 cm per month*, and the skull begins to get thicker. Change is still possible in these older babies, but change is slower and generally requires longer treatment programs. Once a scan is taken, how long will it take to get my child’s cranial remoulding orthosis? Ideally, your child will be fitted with a cranial remoulding orthosis within 14 days of the scanning date to assure proper fit and function. How often will my infant need to see the orthotist for follow-up and/or adjustments? Frequency of follow-up visits usually depends on the severity of the initial head shape, age of the infant, and individual treatment protocols. Typically, the infant is seen a week after the initial fitting and approximately every 2 to 3 weeks thereafter, throughout the course of the treatment program. Younger infants may require more frequent follow up appointments since their heads are growing so rapidly. Author Kirsten Gibson, B-Tech (tut)Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics. Vice Chair of The South African Orthotic Prosthetic Association.
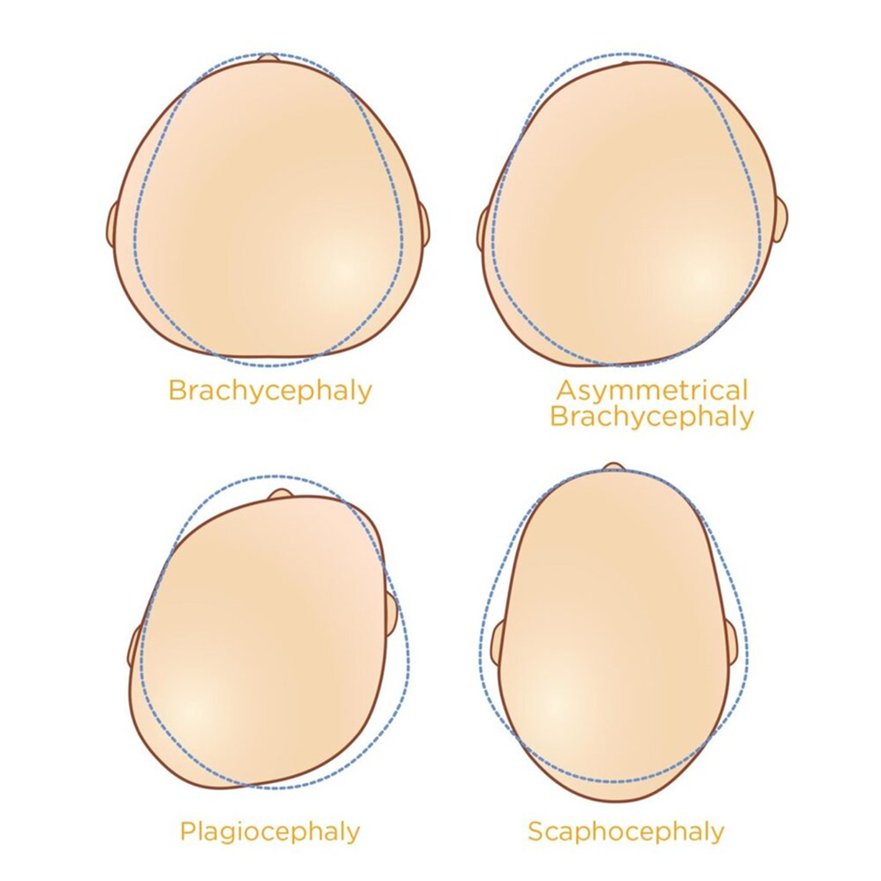
Deformational Brachycephaly Deformational brachycephaly refers to full flattening across the back of the head or flattening at the occipital bone. The anterior-posterior measurement (front to back) appears smaller than the medial-lateral measurement (side to side). The baby’s head appears wider and facial asymmetry is also involved. The area at the top of the head or the cranial vault appears higher. This occurs due to the growth of the baby’s brain accommodating growth in limited space. You may notice that the ears of the baby stick out as well. Deformational Scaphocephaly Deformational scaphocephaly refers to the long, narrow shape caused by the consistent side-lying positioning of the baby. The cranial vault appears high and bossing or prominent areas of growth of the anterior (top) and posterior (back) aspects of the head occur. Our Approach

Our consultations on average take about an hour. During these consultations we assess, measure, scan and fit of the cranial remoulding orthosis/helmet. The initial appointment is getting to know your baby and you as the parent/s or caregivers. We complete a full assessment of your childs’ head shape and discuss the possible methods and avenues of treatment.
We will then discuss the treatment costs and procedures. Once all parties are informed and in agreement, we can complete the scanning of your baby’s head which we then use for the manufacturing and fabrication process. Author Kirsten Gibson, B-Tech (tut)Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics. Vice Chair of The South African Orthotic Prosthetic Association.
A head-shape deformity is generally noticed soon after the birth of your baby, within several days, weeks or months. General healthcare practitioners, and you as the parent/s or caregivers will be able to detect an abnormal head shape and/or asymmetries in the facial features and ears that do not resolve in several days.  We aim for an early initiation to achieve the best outcomes. The ideal age of treatment is 4 to 6 months; however, we can provide a helmet for a baby till the age of 18 months depending on the severity and causative factor. The duration of treatment varies due to the different severities and asymmetries present. The orthotic treatment is often used in conjunction with paediatric physiotherapy, osteopathy, chiropractic’s etc. Author Kirsten Gibson, B-Tech (tut) Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics. Vice Chair of The South African Orthotic Prosthetic Association.
Correcting moderate to severe head-shape deformities to reduce the risk of developing several issues such as delayed developmental milestones, low vision, malocclusion, facial asymmetries, and stunted brain growth. Aids in treatment for torticollis. Provide protection and encourage healing in post-operative craniosynostosis. 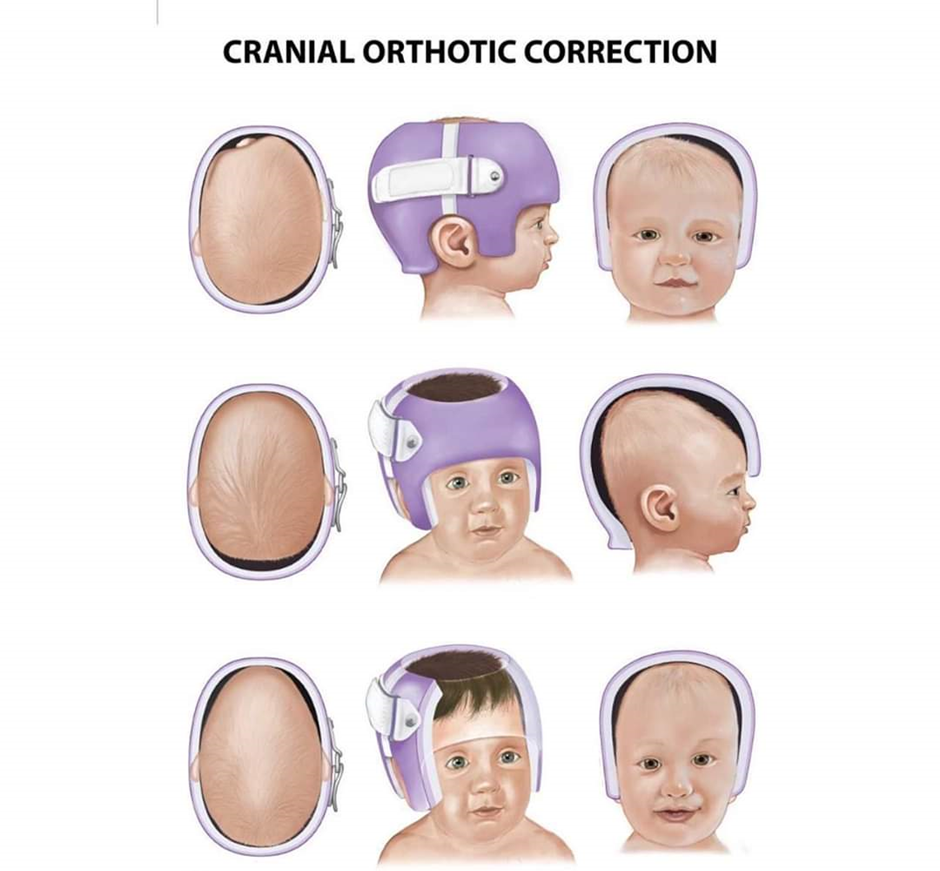 Indications
Contraindications (always check with your healthcare provider)
Author Kirsten Gibson, B-Tech (tut) Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics. Vice Chair of The South African Orthotic Prosthetic Association.
We encounter many individuals who feel as though they have been failed with previous Medical Devices. Often citing that fit and function of their device was poor - not being able to find shoes to wear, the device not being aesthetically pleasing and functionally there being little improvement.  A partial amputation foot can be challenging to manufacture & fit properly. Taking into consideration functional and cosmetic goals, along with patient expectations, wants and needs. The goals when working with our partial foot amputees are to restore stability and function that have been lost due to an amputation, facilitate energy-efficient gait, maintain support, and prevent further complications. At Gibson Orthotics we use modern orthotic and prosthetic techniques and strive to manufacture low profile and aesthetically pleasing devices. Our partial foot amputees are often able to return to a fully functional lifestyle comfortably. Author Kirsten Gibson, B-Tech (tut)Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics. Vice Chair of The South African Orthotic Prosthetic Association.
Flat feet are relatively normal from birth to about two years of age, as the arch doesn’t start to develop until a child starts walking. Even after that, the soles of a child’s feet may look flat, but this does not necessarily indicate a problem. Children with low tone tend to walk late because their feet and ankles are in poor alignment and their toes often claw at the ground for stability, causing their feet to tire quickly. Pronation in children with low tone does not sporadically improve, however it can be managed with a good pair of Orthotics.  These Supra - Malleolar Orthotics are designed to support the feet and ankles, resisting the excessive pronation or flattening of the foot whist children walk. This can be beneficial to patients as it assists in creating a stable base of support for standing, cruising and walking. By doing so we improve stability in the lower limbs and thus improve the patients balance. By supporting your childs feet you are enabling your child to focus on the things that really matter - Play! Author Kirsten Gibson, B-Tech (tut) Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics. Vice Chair of The South African Orthotic Prosthetic Association.
Orthotic devices are shoe inserts that are intended to improve stability and alignment during walking, running and playing. They also can provide positioning for children who are not able to walk or are in the process of learning to walk. But how do you know if your child would benefit from orthotic support? 
If you answered “yes” to any of the above questions, orthotics may be beneficial for your child. Incorrect foot alignment can cause foot, leg, knee, hip and back pain, youth sports injuries, awkward walking or running pattern, poor balance and coordination and toe walking. By using the correct orthotic devices, proper foot alignment can be achieved, resulting in increased balance, coordination and decreased pain. If you believe your child would benefit from orthotic support or if you would like your child evaluated for orthotics, please contact us to discuss your concerns. Author Kirsten Gibson, B-Tech (tut)Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics. Vice Chair of The South African Orthotic Prosthetic Association.
We attended a 2 day course with BLedical to up-skill and add to our Odema treatment toolbox. And boy are we glad we had the opportunity to go! The training helps us enhance patient results, and improve treatment outcomes. Practical hands on experience gained with extensive mobiderm techniques, patient demonstrations as well as personal applications made this course highly beneficial to all attending practitioners.  Click the image for the video Finding the most appropriate and effective compression garment can be challenging for both patient and practitioner, but with guidance from industry leaders and some of the top international compression therapy brands Gibson Orthotics has a solution to meet most patients needs. Author Kirsten Gibson, B-Tech (tut)Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics. Vice Chair of The South African Orthotic Prosthetic Association.
We often get asked “What makes lymphoedema garments so special?” or “ Why cant I just purchase a garment off the shelf from a pharmacy?” Selecting an appropriate compression compression garment can be a challenging task. Many important factors need to be taken into consideration to find the right garment and ensure that perfect fit. As With all of our Medical Devices at Gibson Orthotics - Mobility, Activity, Age, Coverage, General Shape, Diagnosis, Skin Sensitivity & Presentation, Cost and Appearance all have a role to play when selecting the best Compression Garments.  What is the difference between Custom Made and Ready made Garments? The Difference between a higher Quality Compression Garment and a garment of lower quality (Off the shelf varietals) is Fit and compression level. Ready Made Garments are usually made of thin and sheer fabric which are knitted in a circular fashion. They have no seam, or varying yarn tension to create a graduated pressure. Generally Off the Shelf garments are more Cosmetic and lighter in weight. Custom Made Compression Garments are thicker and of higher quality. They have a seam, and measured graduated compression. They are completely customisable, in Length, size, compression colour and fabric - when measured by an experienced professional ensure ultimate fit and comfort. In Order to achieve the greatest results and comfort from a compression garment the appropriate size needs to be correctly measured and selected. If a garment is too small = the Compression is higher than required. If a garment is too big = the Compression is lower than required. With Odema and Lymphoedema patients there is a very fine balance in compression that needs to be achieved to prevent the Oedema worsening. When an individual is measured by a qualified, and experienced Orthotist, the end results are far superior to simply getting a “one size fits all” solution. Call us today to schedule an appointment to discuss your Compression Garment needs! Author Kirsten Gibson, B-Tech (tut)Founder, Director and Senior Orthotist Prosthetist at Gibson Orthotics.
|
AuthorKirsten Gibson owner and founder of Gibson Orthotics is a passionate O & P Clinician with notable experience in Paediatrics and Lymphology. Actively involved in Improving patient and professionals knowledge on the subjects of O & P. Archives
January 2021
Categories
All
|


 RSS Feed
RSS Feed
HOME | OUR VISION | HISTORY | ACCOMPLISHMENTS | CRANIAL ORTHOTICS | CUSTOM ORTHOTICS | COMPRESSION GARMENTS | NEWS
CONTACT US TODAY
OPENING HOURS:
|
|
Practice No: 06702084 | HPCSA Reg No: OS 0008052